{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 kirtleymd@yahoo.com
kirtleymd@yahoo.com
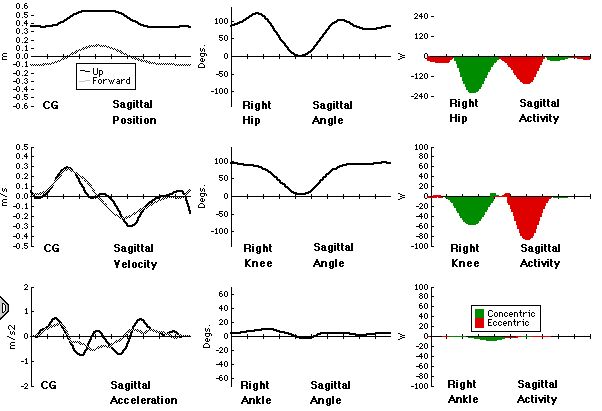
The first action is a controlled falling of the trunk forwards, resisted by eccentric hip extensors. This causes the CG to move forwards of the centre of pressure, at which point standing is initiated. Hip and knee extensors contract powerfully and concentrically to lift the trunk from the chair. Power flows proximally at both hip and knee (with a maximum at 20%), but is largest at the hip, showing that the glutei are most responsible for trunk elevation. Energy of the trunk achieves a maximum at 30% of the duration of the activity, due to a combination of potential and (paradoxically) reversing velocity as it slows to a stop at 40%. During standing the CP is well forward, and a small amount of ankle plantarflexor activity is noted (the ankle musculature being otherwise silent).
The way down is basically the reverse: with hip and knee extensors acting eccentrically to slow the descent of the trunk. Note that again the power flow distally is much larger at the hip than the knee (hip extensors are now more active than knee extensors). Interestingly, the knee compressive force is slightly larger coming down than going up, showing that the knee moment is, in fact, larger but the knee angular velocity lower on sitting down.
The Power Balance curves reveal good balance for the thigh (though slightly less accuracy for the Shank and Foot segments), suggesting that the inverse dynamics calculation is reasonably sound. We expect the curves for power flow into the segments to be a little higher than the measured segment power because the body is not 100% efficient, with a little power being lost along the way.
I have noticed one or two interesting things in the analysis:
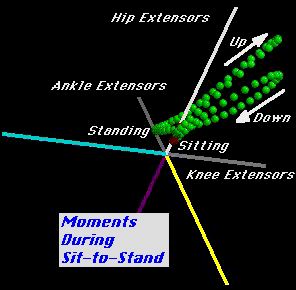
1) More power is generated at the hip during standing, and roughly equal amounts at the hip and knee during descent. This is nicely illustarted in a 3D plot of the moments that I've added to the page.
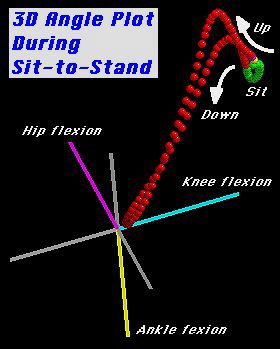
2) A 3D
plot of the angles incidentally shows a sort of hooked trajectory, with
the initial and final hip motion appearing as a small tail on an oitherwise
almost straight line.
One commentator suggested that sit-to-stand begins when the centre of foot pressure (CoP) moves backwards. I think the analysis disagrees with this... in this example (which I think is representative?) the first action is an eccentric flexion of the hip, which has little effect on the CoP (since there is little weight on the ground at this time - the chair is taking most of the weight), but if anything moves it forwards slightly. I suspect this is done to move the CoM forwards of the CoP - perhaps this hip flexion does is not needed if the feet are placed further back (under the chair)... but that would hardly be a natural way to stand.
I look at 4 components when analyzing all movement, based on the working model for movement analysis proposed by Fisher and Yakura: base of support (BOS), alignment, sequencing, and stability/mobility (that is, what segments are stable and what segments are mobile). I will attempt to describe how alterations in these components might change the magnitude of the curves (but perhaps not the proportions) in normal individuals, and perhaps throw in a few thoughts on abnormal sit to stand.
Base of support in sitting generally consists of the ischial tuberosities, posterior femurs, and perhaps the palmar suface of one or both hands. Base of support can be either wide or narrow, large or small. Although I am unaware of any scientific literature to back me up on this, trying it yourself will show that it is more difficult to get up from a wider base of support (e.g. sitting far back on a surface) versus sitting at the edge, and that it is easier to get up from a higher surface (e.g. a barstool) than a lower surface (e.g. a footstool). Clinically I vary these parameters to re-train sit to stand in my patients (particularly post-stroke and brain injured individuals), so I may begin from a higher surface and a narrower base of support, assuming that the temporal-spatial aspects of the movement are similar in all variations of sit to stand and that practicing a variation in which the patient can be successful to promote the necessary strength and
Alignment: again, trying it yourself, it is more difficult to sit to stand maintaining a posterior pelvic tilt than an anterior pelvic tilt. Thus, having adequate hip flexion, lumbar spine extension, thoracic extension, and scapular depression (all components of attaining an anterior pelvic tilt) are important in attaining an optimal initial alignment.
Sequencing: Initiating from a posterior pelvic tilt with lumbar extension/hip flexion rather than thoracic extension (which occurs in the absence of available lumbar range or poor movement habits) is the first desirable motion, and then follow further hip flexion, knee flexion, and ankle dorsiflexion, then hip extension, knee extension, and ankle plantaflexion as one rises to standing.
Stability/Mobility: Initially in sit to stand, the lower extremities are the stable unit, and the pelvis and spine are mobile as ideal starting alignment is attained. Once forward progression begins, this reverses and the trunk is the stable unit, while the lower extremities are the mobile units.
One interesting point Chris made was about center of pressure movement. In normals, I agree that center of pressure moves forward. However, in pathological situations such as stroke and brain injury, it appears to me that center of pressure moves backwards in many cases.
I welcome any comments.
Melanie Weller PTLA, ATC
Sit-to-stand movement can be observed to be occurred in 3 phases - acceleration, transition and deceleration. During initiation, an individual has to generate enough propulsive impulse force in order to bring the body forward. This propulsive force was found to be related to a posterior movement of the COP. This was shown in several studies by employing the force platform. It was clearly shown that the COP moved backward for a few centimeters before it moved forward. Once the subject is off the chair, the COP apparantly lies the sides of the COM. If it was found experimently, there may be some underlying mechanisms that explains this finding. May be that the initial activation is not ecentric hip flexor, although the first action that observed is forward movement of the trunk.
What do you think, looking forward to having your comments.
Margaret Mak Assistant Professor Department of Rehabilitation Sciences Hong Kong Polytechnic University.
Melanie Weller said...
Although I am unaware of any scientific literature to back me up on this, trying it yourself will show that it is more difficult to get up from a wider base of support (e.g. sitting far back on a surface) versus sitting at the edge, and that it is easier to get up from a higher surface (e.g. a barstool) than a lower surface (e.g. a footstool).
So I think we ought to check this out by measuring the joint kinetics in a variety of starting positions:
1) Wide or short base of support
2) High or low seat
...it is more difficult to sit to stand maintaining a posterior pelvic tilt than an anterior pelvic tilt. Thus, having adequate hip flexion, lumbar spine extension, thoracic extension, and scapular depression (all components of attaining an anterior pelvic tilt) are important in attaining an optimal initial alignment.
I propose to use a wedge under the subject to manipulate this variable:
Sequencing... we'll try it out with and without initial hip flexion.
I'm aware that I'm making a fair amount of work for myself, but I'd like to settle these points before we move on.
Let me know what you think, and I'll have a go at the experiments later this week. Or if anyone else would like to volunteer their services...please do! This could be the first science performed over the web - wonderful!
Chris
I have a few comments about the proposal to investigate the effects of base of support and seat height on standing up from sitting.
The effect of seat height has been established in several published reports, including:
Burdett et al (1985). Physical Therapy 65(8): 1177-1183 Ellis et al (1984). J. Biomed. Eng. 6: 113-120 Rodosky et al (1989). J. Orthopaedic Research 7: 266-271 Wheeler et al (1985). Physical Therapy 65: 22-26 Schenkman et al (1996). Clinical Biomechanics 11: 153-158
These studies have demonstrated that, among other things, as seat height is lowered there is increased maximum trunk flexion angular velocity and increased maximum extension velocity of the hip and knee with some changes in the timing of these events. In addition, as chair height is lowered the peak knee extensor muscle moment increases.
In terms on base of support, it is probably the position of the feet (ie. initial ankle dorsiflexion) which is critical. There have been a number of published reports investigating the effects of foot position, including:
Fleckenstein et al (1988). J. Biomech 21: 915-918 Shepherd et al (1996). Scand. J. Rehab. Med 28: 79-88
These studies suggest that if the feet are positioned forward (ie. in less ankle dorsiflexion) there is an increase in the speed and amplitude of forward trunk flexion, as well as an increase in the hip extensor muscle moment. With the feet in a forward position the base of support would be larger than that it the feet were back and the ankles dorsiflexed. So perhaps it is the position of the feet which is important - the buttocks only need to be positioned on the chair so that the chair does not physically block knee extension required for final standing alignment.
Perhaps these studies should be considered before proposals for data collection.
Anne Moseley PhD Student School of Physiotherapy The University of Sydney
Thanks for your very comprehensive commentary on the sit-to-stand laboratory. I certainly appreciate the references, as sit-to-stand is not one of my specialties.
I do wonder, though, why everyone seems to concentrate on velocity and momentum in sit-to-stand whereas in gait we talk about joint and segment powers. I have yet to see an analysis of sit-to-stand published that include joint powers, and it seems to me that these are variables directly describing muscle function.
I will certainly chase up those references. Thanks again for your interest. Are you doing work on this topic yourself?
Best wishes,
Chris
It is interesting how the standing up research does focus on velocity and momentum. One of the reasons for this, I think, is that part of the task occurs with the thighs supported which makes it extremely difficult to calculate joint moments etc. Obviously there are some critical features which occur prior to thighs off, so researchers attempt to characterise them from a kinematic perspective. There are several studies which describe joint moments and velocities after thighs-off (ie. in the extension phase) from which you can derive power.
I have investigated standing up from sitting (along with walking and stair descent) for one of my PhD studies and am currently undertaking a study investigating both successful and unsuccessful attempts to standup. A significant amount of research has been done in the school's laboratory investigating standing up.
As I indicated in my message to the mailing list, it is probably important that the published investigations (about 50 papers!) are reviewed prior to formulating research questions so you don't reinvent the proverbial wheel.
I look forward to ongoing discussions on this topic
Anne Moseley PhD student School of Physiotherapy The University of Sydney PT_MOSELEY@CCHS.USYD.EDU.AU
I'm thrilled to hear you'll be doing such experiments. Let me know how they come out, please. We usually standardize the medial foot border separation, usually at 10 cm, by the way.
Dave
A comment or two on seat height and foot position.
One other study on seat height to add to the list provided by Ms. Moseley was performed at the Massachusetts General Hospital in a patient with a pressure instrumented femoral endoprosthesis (published by Fagerson et al., Physiother (London) 1995, 81:533-540). Acetabular contact pressures were approx. 80% lower when rising from a 62 cm chair compared to rising from a 48 cm chair. Acetabular contact pressures were also 50% lower when rising from the 62 cm chair with the operated leg (the one with the implant) in front of the contralateral leg compared to rising from the same chair with feet together.
Regarding foot position, Pai et al. (Arthritis Rheum 37: 1297-1304, 1994) showed that patients with knee arthritis tend to position their feet further away from the base of the chair, which is likely due to limited ROM (see Fleckenstein et al., J. Biomech 21: 915-918, 1988) rather than attempting to increase base of support. Anyway, the kinetic result is a higher hip extensor moment and a lower knee extensor moment. I found this interesting and had a couple subjects (normal elders) perform sit-to-stand with both feet back (ankle dorsi-flexed 15 deg), both feet mid (ankle 0 deg) and both feet forward (ankle plantar flexed 15 deg). There was indeed an increase in hip extensor moment when the feet were placed further away from the chair, BUT no change whatsoever in knee extensor moment. Has anyone had similar findings?
Ronny
==========================
Chris A. McGibbon (Ronny) PhD Technical Assistant Director MGH Biomotion Lab Boston MA, 02114
Burdett RG Habasevich R Pisciotta J and Simon SR (1985) Biomechanical
comparison of rising from two types of chairs Physical therapy 65:
1177-1183
Rodosky MW Andriacchi TP and Andersson GBJ (1989) The influence of chair
height on lower limb mechanics during rising Journal of Orthopaedic
Research
7: 266-271
Regards
Peter Roche
Clinical Manager Physiotherapy
Ballarat Health Services
PO Box 199
Ballarat VIC 3353
Phone: (03) 5320 3963
Fax: (03) 5320 3800
E-mail: peterR@bhs.grampianshealth.org.au
Like to know more, or criticise my methods? Email me!
kirtleymd@yahoo.com