First, I think that there are problems with the right side in addition
to
the left side. I think primarily there is spasticity
in the right side,
which is preventing a proper pelvic obliquity curve. This
is
leading to a partially 'crouched' gait for the right hand side.
It is hard
to identify exactly which muscle is causing this problem, but could
be a
combination of both spasticity in the hamstrings and the rectus
femoris.
I would like to know where on the left side the Botox is being administered.
Thanks
Richard Williamson
Department of Biomedical Engineering
phone (403)492-0723
University of Alberta, Edmonton AB
(403)471-2262 ext 2688
T6G 2J5
fax (403)492-8259
My thanks to Richard Williamson for starting us off on this one. Also to Yves Blanc in Geneva for pointing out to me privately that my ASIS markers on this patient were attached to her clothing. With great humility, I agree with him that this would likely lead to dubious results in view of the great sensitivity of the Davis model hip-joint calculation to ASIS placement. However, it occurs to me that we might not be the only culprits to fall foul of this shortcut, so I thought I'd pass his comment on for public consumption (and my castigation!).
Both Richard and Yves also ask for more clinical details on this case, which I agree are required. She's coming in for the post-Botox analysis with her physio on Thursday, so I promise to add these to the page then, along with the results from the new analysis (hopefully with correctly placed markers!). I thought it might be a useful exercise, though, to try to come to a conclusion about the diagnosis with only the biomechanics to work with and without knowing too much about the clinical examination.
Chris
--
Dr. Chris Kirtley MD PhD
Dept. of Rehabilitation Sciences
The Hong Kong Polytechnic University
Hong Kong
We are engineers from the gait laboratory of Politecnico di Milano,
Italy;
we saw your gait analysis database on the web and we'd like
to know how to
insert our data to your database.
We are interested also in comparing our data with yours, since we acquire
our data with a different system (Gaitel 20 by Bts, Italy).
Looking forward to your advice
Best regards
Ing. Mattia Vierzi and Ing.
Federica Sibella
"L. Divieti" Gait Lab
Bioengineering Dept., Politecnico di Milano, Italy
Comment on the hemi or diplegic gait:
It seems that both sides were involved, however it was more obvious
at the left side.
The knee flexion in the initial contact of left foot was exaggerated,
it may resulted from the
hypertonicity of the calf muscle, properly the gastroc. The increased
in knee flexion helped to
reduce the stretching on the calf during the loading response, hence
reducing the equinus
deformity at the ankle joint. On the other hand, anterior
movement at the upper body was mainly
accompanied with the extension of the knee but little tibia advancement
over the foot just after
the double support period.
The gastroc may be considered as weakness in eccentric component
which is essential in
controlling the advancement of the tibia over the ankle as appear
in normal gait.
I think the child has higher chance to walk with hyperextended
knee during the mid-stance if the
eccentric control of the gastro or the calf was not enhanced.
I think Botox injection will only weaken the muscles if gastroc was
a target! The ankle stability
will be ruined. Two secondary compensation may result:
Dicky Wong
Physiotherapist , Pamela Youde Nethersole Eastern Hospital
Hong Kong
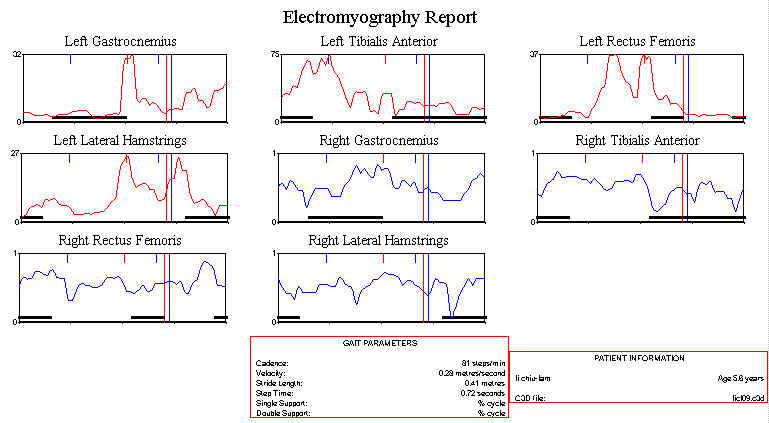
I'd like to respond to the comments made so far. I think they raise
some
interesting questions.
Richard Williamson suggested that co-contraction of rectus and
hamstrings might be causing a crouch type gait. Indeed, there
does seem
to be coactivation, as you can see in the EMG at:
She still walks with a flexed knee at contact, although the jump
knee
has now improved. Thus, I wonder if the next step might be injection
of
Botox into the hamstrings? The knee is also limited a little in its
swing, so I guess one might also want to inject the rectus. I haven't
heard of that being used very often - is there a reason for that? What
are the other possibilities for the knee - physical therapy? electrical
stimulation? surgery??? Also, will the gastroc Botox have to be repeated
every few months, or will there be some sort of carry-over effect?
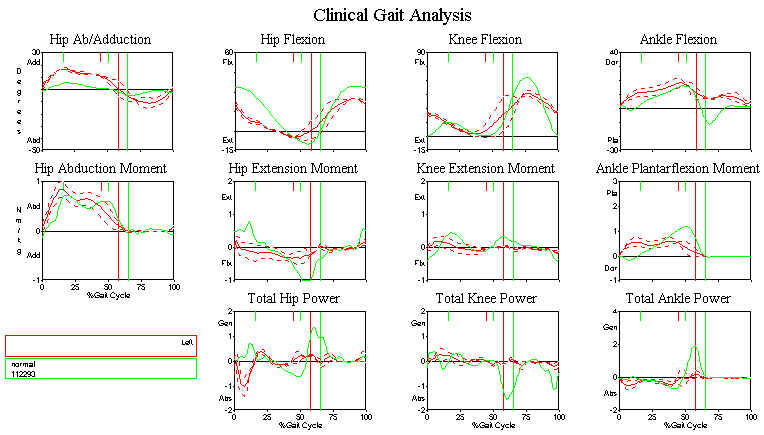
What about Dicky's anxiety about Botox causing weakness? It's
of
interest to me that the A2 push-off power - see
/archives/16-7-99/poleftkn.jpg
- has
virtually disappeared since the injection, so how is she walking faster
then? There doesn't seem to be any compensatory increase in any of
the
other joints, except, perhaps for an increased K2 at the knee.
So I
still don't think we know why the Botox has worked.
Everyone seems to agree that there are problems on both sides, and one
putative diagnosis would be "Bilateral Hemiplegia". A last question
I
would like to pose, then, is: how can we differentiate between a
diplegia and a bilateral hemiplegia from the gait analysis results?
Look forward to your thoughts,
Chris
--
Dr. Chris Kirtley MD, PhD
Assistant Professor
Department of Rehabilitation Sciences
The Hong Kong Polytechnic University
I thought this private query merited a public response. Please feel
free
to disagree with my definitions.
Chris,
I've been following the current case of the week and I just had a couple
of questions. There are a few terms that you use with
which I am not
familiar.
I've looked in some of my texts and still have not found an explanation
for them. I was hoping that you could explain what they mean
or give me
some references to get the info myself.
Here they are:
1. jump knee
2. A2 push-off power
3. K2 at the knee
Good point - I guess we need a glossary on the CGA site. Here goes:
1. Jump knee - interesting term really. It's an old clinical
expression,
which basically means that the leg lands with a flexed knee, which
then
extends in stance phase before flexing again in swing (giving the
impression of 'jumping'). This is contrast, of course, with the normal
knee, which is extended at contact, before flexing slightly during
stance (stance phase flexion). The flexed knee at contact is indicative
of tight hamstrings and/or gastrocnemius, which prevent the knee from
extending in terminal swing. The abnormal extension during stance (often
hyperextension) is, I believe, usually due to weak quadriceps, which
prevents the normal stance phase flexion. Absence of stance phase
flexion (absent loading response) on its own is seen in a great many
disorders in which there is weak quadriceps or knee pain (in which
the
quadriceps contraction is avoided to minimise bone-on-bone joint
compressive force).
2. A2 push-off power - the large concentric power burst (about
1-3 W/kg
normally) occuring prior to toe-off - the main power responsible for
propelling the leg forwards into swing. Note, however, that very little
of this power is transmitted proximal to the knee, so push-off does
not
push the trunk forward (as is sometime wrongly assumed). Also, Dr.
Chen
in Taiwan has shown that as speed increases, the relative contribution
of ankle push-off to forward power (the sum total of
all the
concentric power bursts) falls from over 60% to around 50%, with knee
(K2) and (more especially) hip (H1,3) taking over (as they do in
patients who have reduced push-off).
3. K2 at the knee - the concentric power generated by the quadriceps
during stance phase, when the knee is extended again after undergoing
its stance phase flexion during loading. It contributes only about
10-15% of forward power during normal gait, but may be an important
compensatory power in patients. The table below summarises the various
contributions:
Speed Ankle Knee Hip
Total Forward Power
Slow 0.22 0.04
0.08
0.35
(63%) (11%) (23%)
Normal 0.21 0.06
0.12
0.39
(54%) (15%) (31%)
Fast 0.19
0.10 0.15
0.45
(42%) (22%) (33%)
(Values in J/kg body mass)
Chen et al, Gait & Posture 6: 171 - see also
Winter DA (1991) The biomechanics and motor control of human gait:
normal, elderly and pathological. University of Waterloo press, Ontario.
I'd be interested to hear what people think of the idea of "forward
power", and the whole business of joint power - I know it's still a
controversial subject!
Chris
--
Dr. Chris Kirtley MD, PhD
Assistant Professor
Department of Rehabilitation Sciences
The Hong Kong Polytechnic University
I just gave a quick look at the results of the current case of the week.
Here are some thoughts.
It seems to me that your patient may be walking faster due to the
delayed H1S power generation peak by the hip extensors. I believe
that this peak
has the potential to be more effective and get the patient to move
faster
based on the fact that it appears at mid stance. However this peak
is hardly
explained as a hip extensor generation based on the hip moment and
angle
graph above. I wanted also to point out the absence of or
the
ineffective H2S hip flexor absorption at the late stance. In
addition, it seems that
there is a great deal of frontal plane movement at the hip that
she may
be taking advantage of to move forward.
Further to your "challenge":
I'd be interested to hear what people think of the idea of "forward
power", and the whole business of joint power - I know it's still
a
controversial subject!
From a strictly mechanical point of view, power is a a dot (i.e.
scalar) product. It can therefore have no direction (not up,
not
down, not flexor, and certainly not forward!) but only a sense
(either positive, also referred to as "generated", or negative, also
referred to as "absorbed"). In this regard, VCM (as I recall), is
guilty of breaking up joint power into different "components",
suggesting that power is a vector which of course it is not.
As we have shown (cf. Gait & Posture, 5:204-210, 1997), power
is very
dependent on the model that you use. Personally, I am dubious
of the
accuracy of joint power data (depending as it does on the derived
parameters joint moment and joint angular velocity which are
notoriously noisy), and so my own advice to anyone using the Winter
approach of A2, K3, etc. is "watch out"!
Kit
Vaughan
University of Cape Town
{kind=link}
{kind=link}